During the 2026 International Confederation of Midwives (ICM) Congress in Lisbon, an important debate unfolded—one that reached far beyond conference halls and professional organizations. It sparked conversations across the global birth community about recognition, regulation, cultural knowledge, and the future of maternity care.
At the centre of the discussion was the temporary suspension of the ICM's 2021 Position Statement on Partnership Between Indigenous and Non-Indigenous Midwives, pending a review. The ICM explained that the review was intended to ensure consistency with its definition of a regulated midwife and to clarify terminology. However, many Indigenous midwives, advocates, and organizations experienced the decision differently. For them, suspending the only position statement specifically acknowledging Indigenous midwifery felt like losing an important recognition of their place within the global birth community.
Whether one agrees with the decision or not, the debate raises a much larger question:
Who gets to decide what counts as knowledge?
Birth Did Not Begin With Modern Medicine
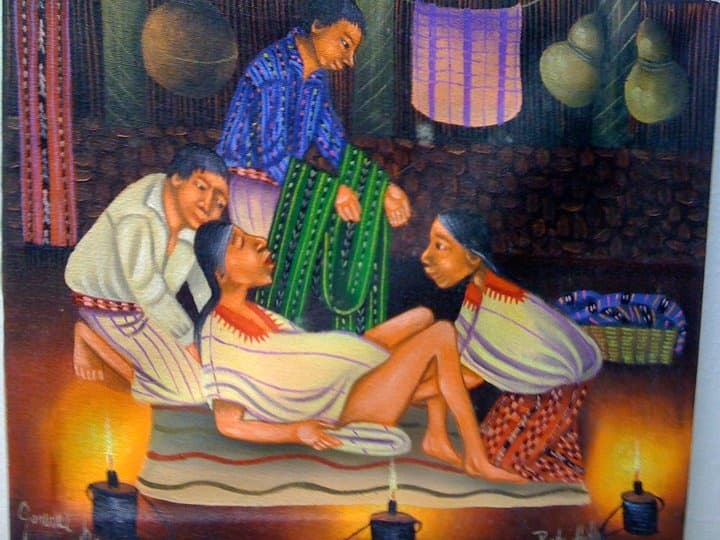
For thousands of years, long before hospitals existed, women gave birth in their communities.
They were accompanied by experienced birth attendants who learned through apprenticeship, observation, mentorship, and generations of accumulated knowledge. This knowledge was rarely written in textbooks. It lived in stories, hands, relationships, and experience.
Today, Indigenous midwives continue to care for women in many parts of Latin America, Africa, Asia, Oceania, and other regions of the world. Many provide care that extends beyond labour itself, supporting pregnancy, postpartum recovery, breastfeeding, family wellbeing, and community traditions.
Their work is deeply rooted in the realities of the communities they serve.
They know the language.
They understand local customs.
They recognise subtle changes in mothers because they often care for entire families across generations.
This is a form of expertise that deserves to be understood rather than dismissed.
Why Regulation Matters
Recognising Indigenous knowledge does not mean rejecting modern medicine.
On the contrary.
The progress made in maternal and newborn healthcare over the last century has saved countless lives. Safe caesarean birth, antibiotics, blood transfusions, neonatal intensive care, emergency obstetrics, and evidence-based clinical practice have dramatically reduced maternal and infant mortality.
Professional education, regulation, and accountability are essential.
They protect women.
They protect babies.
They protect the profession itself.
These standards should never be abandoned.
Likewise, not every traditional practice should automatically be preserved simply because it has existed for generations. History reminds us that some practices have caused profound harm. Female genital mutilation, including forms such as infibulation, is one example. Cultural traditions, like modern medical practices, must always be examined through the lenses of human rights, safety, ethics, and informed consent.
Respect for Indigenous cultures does not require idealising every tradition.
It requires thoughtful discernment.
Exclusion Is Different From Discernment
Rejecting harmful practices is not the same as rejecting an entire body of knowledge.
This distinction matters.
Too often, Indigenous midwives have been viewed as if the absence of a university degree means the absence of expertise.
But knowledge can be acquired in different ways.
Some knowledge is learned through formal education.
Some through supervised clinical training.
Some through decades of accompanying birth, observing patterns, recognising complications, and caring for families over generations.
A university qualification is one important way of validating professional competence.
It is not the only way human beings acquire wisdom.
Rather than asking whether Indigenous midwives should replace regulated healthcare professionals, perhaps we should ask a different question:
How can their knowledge contribute alongside modern healthcare while maintaining high standards of safety and accountability?
In Many Places, Indigenous Midwives Are the Maternity System
This debate is sometimes framed as though women can simply choose between an Indigenous midwife and a hospital.
For millions of families, that is not reality.
In many remote communities, hospitals may be several hours away.
Roads may become impassable during certain seasons.
Healthcare professionals may be scarce or completely absent.
For these communities, Indigenous midwives are often the only people available to provide continuous care during pregnancy and birth.
The answer cannot simply be to declare that these women are not recognised because they lack formal credentials.
That does nothing to improve maternal health.
A more meaningful response would be to strengthen collaboration:
creating respectful referral pathways when complications arise;
offering continuing education while respecting local knowledge;
improving communication between hospitals and community birth attendants;
ensuring access to emergency care without forcing communities to abandon their cultural identity.
Supporting Indigenous midwives does not mean lowering standards.
It means expanding support.
Science and Traditional Knowledge Are Not Enemies
Modern science has transformed healthcare because it continually asks questions, evaluates evidence, and improves practice.
That same openness should allow us to engage respectfully with traditional knowledge.
Not every ancestral practice should be accepted.
Not every biomedical practice is beyond criticism.
Both traditions evolve.
Both benefit from humility.
The goal should never be to place one system above the other.
The goal should be to build relationships where knowledge can be shared, questioned, strengthened, and improved—for the benefit of mothers, babies, and families.
Looking Forward
The debate that emerged in Lisbon is about far more than terminology.
It asks us to consider what kind of maternity care we want for future generations.
Do we build systems that recognise only one pathway to knowledge?
Or do we create systems where scientific education, professional regulation, lived experience, cultural wisdom, and community relationships can coexist while remaining accountable to the highest standards of ethics and safety?
The future of birth care is not served by exclusion.
It is served by collaboration.
By listening before judging.
By recognising that protecting women requires both excellent healthcare and culturally respectful care.
No single profession, culture, or institution holds all the answers.
The mothers and babies of the future deserve the very best that every tradition—scientific and ancestral alike—has to offer.
References
International Confederation of Midwives. Statement on the Temporary Suspension of the Position Statement on Partnership Between Indigenous and Non-Indigenous Midwives (2026).
World Health Organization. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience (2018).
World Health Organization. WHO Recommendations on Maternal and Newborn Care for a Positive Postnatal Experience (2022).
United Nations Population Fund (UNFPA). State of the World's Midwifery 2021.
International Confederation of Midwives. International Definition of the Midwife.
The Lancet. The Lancet Series on Midwifery (2014).
United Nations Educational, Scientific and Cultural Organization (UNESCO). Convention for the Safeguarding of the Intangible Cultural Heritage (2003).



